My name is Rebecca Sowards and I am a declared Recreational Therapist major at the University of Utah. In 2010, I joined a local non-profit organization called "Good in the Hood", which focuses on reaching out and building our communities. The time I spent within my surrounding communities were some of the most rewarding experiences I’ve ever had and they really ignited a spark in me to participate in service. Over the years my passion for reaching out to others has evolved into an emphasis of individuals with disabilities. I had the opportunity to intern for Utah's chapter of the Make-A-Wish Foundation, which was unforgettable. Witnessing the process of a child's wish coming true and to be involved in the wish process was something unexplained. However, at the end of the internship, I realized I wanted more of a one-on-one interaction with children with disabilities. When I selected Recreational Therapy as my professional route, not knowing much about it, I was pleasantly surprised at how much I agreed with its practice.
Recreational Therapy, an impacting process, focuses on assessed and individualized needs of those with an illness or disabling condition. A Certified Therapeutic Recreational Specialist (CTRS) is a trained mentor that assesses, plans, and implements recreational or activity-based interventions. She/he sets goals and objectives to break down preventing barriers and provides resources to achieve an overall physical, psychological health, recovery, and well-being. Recreational Therapy is my passion because it considers "health" more than just the absence of "illness". Recreational therapy gears towards empowering individuals to participate in full and independent life pursuits through its use of recreational modalities.
The Self-Determination Theory
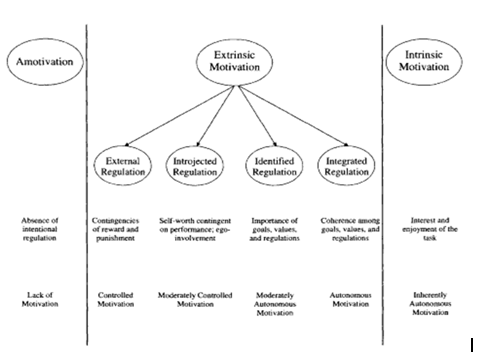
The Self-Determination Theory (SDT) is a theory rooted in motivation. It is concerned about the very nature or intrinsic tendencies of influencing behavior in effective and healthy ways (Gagné and Deci, 2005). The theory looks at the motivation behind the choices people make without external influences and interferences. It focuses on the degree to which an individual’s behavior is self-motivated and self-determined (Ryan and Deci, 2007).
The SDT uses a continuum model. It ranges from amotivation, which is basically lacking in self-determination, to intrinsic motivation, which is invariably self-determined (Ryan and Deci, 2007). Between amotivation and intrinsic motivation, along the descriptive continuum, are the four types of extrinsic motivation; external, interjected, identified, and integrated (Figure to the Right).
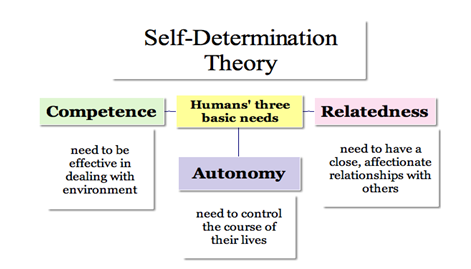
The self-Determination Theory is centered on a belief that humans have an intrinsic nature to show persistent positive features such as, effort, agency, and commitment to their own lives (Wehmeyer and Schalock, 2004). Each individual also has innate psychological needs that make up the foundation for their self-motivation and personality integration. Three of these innate needs necessary for function and growth include; competence, relatedness, and autonomy (Figure Below).
How does Self-Determination relate to Recreational Therapy?
Participants are more likely to benefit from recreational therapy services if they are intrinsically motivated to participate. With the thousands of individuals with disabilities engaging in the therapy process, mechanisms that support participation are crucial in receiving positive outcomes and improving quality of lives. Those who utilize the SDT, will help participants become intrinsically motivated and self-determined. These individuals are more likely to be engaged in behavior change settings and continue to engage in behaviors after the close of treatment. Furthermore, as a TR specialist builds rapport with a client, the basis need of relatedness, becomes strengthened and continues to grow though interactions with multiple group settings.
Where is Self-Determination applied in Recreational Therapy?
“Individuals who are intrinsically motivated in certain situations are more likely to learn, adapt, grow in competencies that characterize development” (Ryan and Deci, 2007). In order for TR goals to be successful, participants need to be able to grow, learn, and adapt. When individuals are intrinsically motivated to do so it becomes a very valuable and helpful factor in their treatment process. Although therapists may apply only portions of the theory at times, intrinsic motivation is considered a required element for leisure. Many therapeutic recreation practice models, including the, Leisure Ability Model, TR Service Delivery and Outcome Models, and the Leisure and Well-Being Model all incorporate intrinsic motivation as an important piece. The emphasis and prevalence of this intrinsic motivation in these models demonstrates its importance in the TR process. In other words, the Self-Determination model’s existence in practice should be more recognized and understood than it currently is as it plays a key part in the leisure experience and supporting autonomy, competence and relatedness of its participants.
Author’s Purpose: Youth in residential mental health facilities often have a history of significant traumatic experiences that significantly impacted their perception of healthy relationships. They were either not provided with healthy role models or learned from abusive relationships with peers, adults, family members. The youth therefor lack the understanding of what a successful healthy relationship is and how to nurture it. A music therapist, CRTS, and the author of this article, teamed up to develop an anti-bullying program that uses the APIED process to help improve a common goal; “To improve the ability to establish and maintain healthy relationships”. The program is developed through websites and other resources that address bullying.
“Help youth learn what bullying behavior is, how to interact with others in a healthy way, and how to stand up for others who are victims of bullying behavior” (page 2).
Key Program Elements:
I. Youth were assessed by a ST interview/leisure inventory, a specialized assessment, trauma inventory, and an Ansel-Casey Life Skills assessment.
II. Pre and-Post-test (short answer questions) for the counseling groups will occur.
III. A specialized treatment plan was formed for each in the group (goals and objectives)
IV. Available resources; web-based, books, videos, lectures.
V. Intervention occurred once a week for 30-45 minutes over eight weeks depending on the amount of youth in the group and their individual needs.
VI. 8 week sessions follow a detailed program outline of planned activities with protocols.
VII. After each group program the group will discuss and evaluate the session.
VIII. Informative and summative documentation.
Key Claims or Propositions:
- The Anti-bullying group has proved to be a valuable group in teaching youth about;
- Unhealthy characteristics in relationships (bullying behaviors)
- Different types of bullying
- How to stop bulling by not passively watching
- Learning assertiveness skills to manage bullying behaviors
- Developing empathy for others
- Coping skills to manage situations that involve bullying.
- The Anti-Bullying program is successful due to the Leisure Ability Model it uses and the APIED Process (page 7).
- The learning experiences and selected interventions should address (page 8);
- Functioning deficits
- Regulating emotions
- Following directs’
- Perspective-taking skills
- Acquiring and establishing coping skills
- Establishing and maintain healthy relationships
- The Anti-bullying program will help youth experience healthier relationships in the future (page 8).